 Menu
Note. Scroll up to view more topics.
Menu
Note. Scroll up to view more topics.
 Home
Home
 Contact Us
Contact Us
 STUDY SKILLS
STUDY SKILLS Skills of effective study
Making study-notes
Group Discussion
How to concentrate
Developing interest in study
Making preparation for exam
Test Taking Strategies
How to relieve Exam stress?
Time Management for studies
Attempting Computer-based Exam
How to sharpen your brain?
Causes of failure in Exam
Exam-format-wise Preparation
Parents’ Role in Child’s Education
How to improve memory power?
ENGLISH BASICS Noun and its Types
Countable and Uncountable Nouns
Clause
Types of Clauses
Phrase
Types of Phrases
Phrase & Clause - Difference
Verb - Formation & forms of Verbs
Main Verb and Auxiliary Verb
Transitive and Intransitive Verb
Adjective
Comparative and Superlative
Adverb - Use & Formation
Types of Adverb
Pronoun
Types of Pronoun
Prepositional Verb
Coordinating & Subordinating Conjunctions
English Tenses
Active & Passive Voice
Direct & Indirect Narration
TEST PREPARATION IELTS Exam Preparation Guide
CSS Exam, Pakistan
NTS Test (NAT-I, II & GAT)
GRE General Test
MCAT - Medical College Aptitude Test
Entertainment - Funny Jokes Related Topics
Effects of Thiamine Deficiency
Vitamin B2 – Role & Deficiency
Nicotinamide –Occurrence, Deficiency
Vitamin B6 – Occurrence, Deficiency
Vitamin B5 – Role & Deficiency
Biotin – Occurrence, Role, Deficiency
Folic Acid (FA) or Pteroyglutamic Acid
Symptoms of Vitamin B12 Deficiency
Vitamin C – Changes to it in body
Vitamin A – Occurrence & Absorption
Vitamin K – Occurrence & Absorption
Skills of effective study
Making study-notes
Group Discussion
How to concentrate
Developing interest in study
Making preparation for exam
Test Taking Strategies
How to relieve Exam stress?
Time Management for studies
Attempting Computer-based Exam
How to sharpen your brain?
Causes of failure in Exam
Exam-format-wise Preparation
Parents’ Role in Child’s Education
How to improve memory power?
ENGLISH BASICS Noun and its Types
Countable and Uncountable Nouns
Clause
Types of Clauses
Phrase
Types of Phrases
Phrase & Clause - Difference
Verb - Formation & forms of Verbs
Main Verb and Auxiliary Verb
Transitive and Intransitive Verb
Adjective
Comparative and Superlative
Adverb - Use & Formation
Types of Adverb
Pronoun
Types of Pronoun
Prepositional Verb
Coordinating & Subordinating Conjunctions
English Tenses
Active & Passive Voice
Direct & Indirect Narration
TEST PREPARATION IELTS Exam Preparation Guide
CSS Exam, Pakistan
NTS Test (NAT-I, II & GAT)
GRE General Test
MCAT - Medical College Aptitude Test
Entertainment - Funny Jokes Related Topics
Effects of Thiamine Deficiency
Vitamin B2 – Role & Deficiency
Nicotinamide –Occurrence, Deficiency
Vitamin B6 – Occurrence, Deficiency
Vitamin B5 – Role & Deficiency
Biotin – Occurrence, Role, Deficiency
Folic Acid (FA) or Pteroyglutamic Acid
Symptoms of Vitamin B12 Deficiency
Vitamin C – Changes to it in body
Vitamin A – Occurrence & Absorption
Vitamin K – Occurrence & Absorption
- Home
- Study Skills
 Skills of effective study Making study-notes Perseverance in study How to concentrate Developing interest in study Group Discussion - Importance Where to study? When to study? Start your study now Making preparation for exam
Preparation according to exam-format
Test Taking Strategies
How to relieve Exam stress?
How to take Computer-based Exam
Making study-notes for exam? Why do students get less marks?
Skills of effective study Making study-notes Perseverance in study How to concentrate Developing interest in study Group Discussion - Importance Where to study? When to study? Start your study now Making preparation for exam
Preparation according to exam-format
Test Taking Strategies
How to relieve Exam stress?
How to take Computer-based Exam
Making study-notes for exam? Why do students get less marks?
- English Basics
Articles
Sentence
Subject, Predicate & Object
Kinds of Sentence (Function-wise)
Kinds of Sentence (Structure-wise)
Phrase & Clause – Comparison
Phrase
Clause
High Frequency words - English
English Tense – Meaning
Present Simple Tense
Present Continuous Tense
Present Perfect Tense
Present Perfect Continuous Tense
Past Simple Tense
Past Continuous Tense
Past Perfect Tense
Past Perfect Continuous Tense
Future Simple Tense
Future Continuous Tense
Future Perfect Tense
Future Perfect Continuous Tense
Active & Passive Voice – Meaning
Passive Voice for Tenses
Passive Voice for Modals
Rules for Imperative Sentences
Sentences which can’t be changed
Direct & Indirect Narration – Meaning
Indirect Speech for Tenses
Rules for Interrogative Sentences
Indirect Speech for Modals
Rules for Exclamatory & Imperatives
Rules for change in Pronoun & Time
- Test Preparation
- Resources
- Contact Us
- Entertainment
- Jobs
- News
Vitmain B1 (Thiamine)
(Aneurine, Vitamin B1, Anti-neuritic or Anti-beriberi factor)
 Properties of Vitamin B1
Properties of Vitamin B1
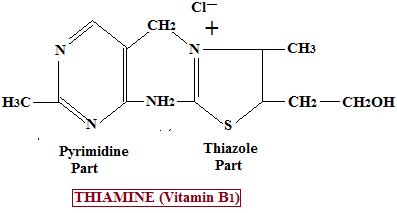
Thiamine is a water-soluble vitamin belonging to the B-complex group. It is a white, crystalline compound with good solubility in water, which makes it readily absorbed in the gastrointestinal tract but also poorly stored in the body.
Chemically, thiamine consists of a pyrimidine ring and a thiazole ring linked by a methylene bridge, a structure essential for its biological activity.
It is heat-labile, meaning it is sensitive to heat, and is slowly destroyed by moist heating, especially during prolonged cooking. However, it is relatively stable when cooking temperatures do not significantly exceed 100°C.
Thiamine is also highly sensitive to alkaline conditions, where it undergoes rapid degradation, particularly when heat is applied. In contrast, it remains comparatively stable in acidic environments, which is why acidic foods and gastric conditions do not significantly destroy it.
It has a mild characteristic odor resembling yeast, reflecting its abundance in yeast-rich foods and microbial sources.
Occurrence of Thiamine (Vitamin B1)
Thiamine is widely distributed in both plant and animal foods, but its concentration varies significantly depending on food processing.
It is present in highest concentration in the outer layers of cereal grains, particularly in bran and rice polishings. During milling, these outer layers are removed, leading to a major loss of thiamine content in refined foods.
Rich dietary sources include whole grains, legumes, nuts, yeast, beef, and liver, which together form the most reliable sources for meeting daily requirements. In contrast, eggs, fish, and most vegetables contain relatively lower amounts.
Highly refined products such as white flour, polished rice, and processed breakfast cereals are markedly deficient in thiamine due to removal of the vitamin-rich outer layers during processing. This nutritional loss is a major contributor to deficiency in populations relying heavily on refined carbohydrates.
Milk contains only small amounts of thiamine, but because of its volume of consumption in some diets, it can still contribute modestly to intake. Intestinal bacterial synthesis of thiamine occurs in humans, but it is not considered a significant or reliable source for meeting physiological requirements.
Absorption, Transport, and Storage
Thiamine is absorbed mainly in the jejunum and ileum. Absorption occurs through a dual mechanism:
- At low physiological concentrations, it is absorbed by an active transport system, which is carrier-mediated and energy-dependent.
- At higher concentrations, absorption occurs via passive diffusion.
After absorption, thiamine is transported in the bloodstream and taken up by tissues where it is rapidly phosphorylated to its active forms.
The body has very limited storage capacity for thiamine, typically sufficient only for a few weeks. It is stored mainly in metabolically active tissues such as the liver, heart, kidneys, and skeletal muscles. Due to this limited storage, continuous dietary intake is essential to prevent deficiency.
Biochemical Role of Thiamine
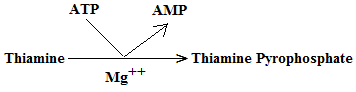
Thiamine exerts its physiological functions after conversion into its active coenzyme form, thiamine diphosphate (TDP), also known as thiamine pyrophosphate (TPP).
This conversion occurs through ATP-dependent phosphorylation, making TPP the biologically active form responsible for most enzymatic actions of thiamine.
TPP functions as a coenzyme (cocarboxylase) for enzymes involved in oxidative decarboxylation and carbohydrate metabolism, particularly α-keto acid decarboxylation reactions.
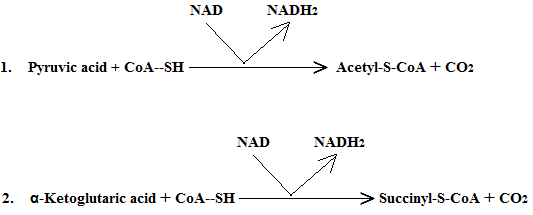
It plays a critical role in energy metabolism by acting as a coenzyme for the following key enzyme complexes:
- Pyruvate dehydrogenase complex
Converts pyruvate into acetyl-CoA, linking glycolysis to the citric acid cycle and enabling aerobic energy production. - α-Ketoglutarate dehydrogenase complex
Participates in the citric acid cycle by catalyzing the conversion of α-ketoglutarate to succinyl-CoA. - Branched-chain α-ketoacid dehydrogenase complex
Involved in the catabolism of branched-chain amino acids such as leucine, isoleucine, and valine.
Through these reactions, thiamine is essential for aerobic glucose metabolism and energy production, particularly in tissues with high metabolic demand such as the brain and heart.
In addition to its role in oxidative decarboxylation, TPP also acts as a coenzyme for transketolase, an enzyme of the pentose phosphate pathway (PPP). This pathway is important for:
- Generation of NADPH, required for reductive biosynthesis and antioxidant defense
- Production of ribose-5-phosphate, essential for nucleotide and nucleic acid synthesis
Because of this role, erythrocyte transketolase activity is used as a functional indicator of thiamine status, and its reduced activity is a sensitive marker of deficiency.
Clinical Importance and Deficiency Manifestations
Thiamine deficiency leads to a spectrum of clinical disorders collectively known as beriberi, as well as serious neurological complications.
The major deficiency conditions include:
- Dry beriberi: This form primarily affects the peripheral nervous system. It is characterized by peripheral neuropathy, muscle weakness, wasting, and reduced reflexes, reflecting impaired neuronal energy metabolism.
- Wet beriberi: This form predominantly involves the cardiovascular system and is characterized by peripheral edema, cardiomegaly, tachycardia, and high-output heart failure, resulting from impaired myocardial energy production.
- Wernicke encephalopathy: An acute neurological emergency caused by severe thiamine deficiency. It is classically characterized by the triad of confusion, ataxia, and ophthalmoplegia. Immediate treatment is essential to prevent permanent damage.
- Korsakoff psychosis: A chronic neuropsychiatric condition often following untreated Wernicke encephalopathy. It is characterized by severe memory impairment, confabulation, and learning difficulties.
Thiamine deficiency is most commonly seen in chronic alcoholism, due to poor dietary intake, impaired absorption, and reduced hepatic storage. It may also occur in malnutrition, prolonged vomiting, starvation states, hyperthyroidism, pregnancy, and conditions with increased metabolic demand.





Copyright © 2023. STUDYANDEXAM. All Rights Reserved.